Muscle-sparing hip replacement through the front of the hip, most patients walk the same day.
The anterior approach to total hip replacement is performed through a small incision on the front of the hip. Rather than cutting through muscle, as is done in the posterior approach, the surgeon works between the natural intervals between muscles, leaving the hip's stabilizing structures fully intact.
For the right patient, this translates into a noticeably faster recovery. The muscles that control walking, stair-climbing, and balance are never detached or cut, so they do not need to heal. Most patients are up and walking the day of surgery, off narcotics within days, and cleared to drive within two weeks.
A CT scan of your hip is used to build a patient-specific 3D model. Implant size, position, and leg-length correction are planned in software before you reach the operating room.
A 3–4 inch incision is made on the front of the thigh. The surgeon works between the sartorius and tensor fasciae latae muscles, no muscles are cut or detached.
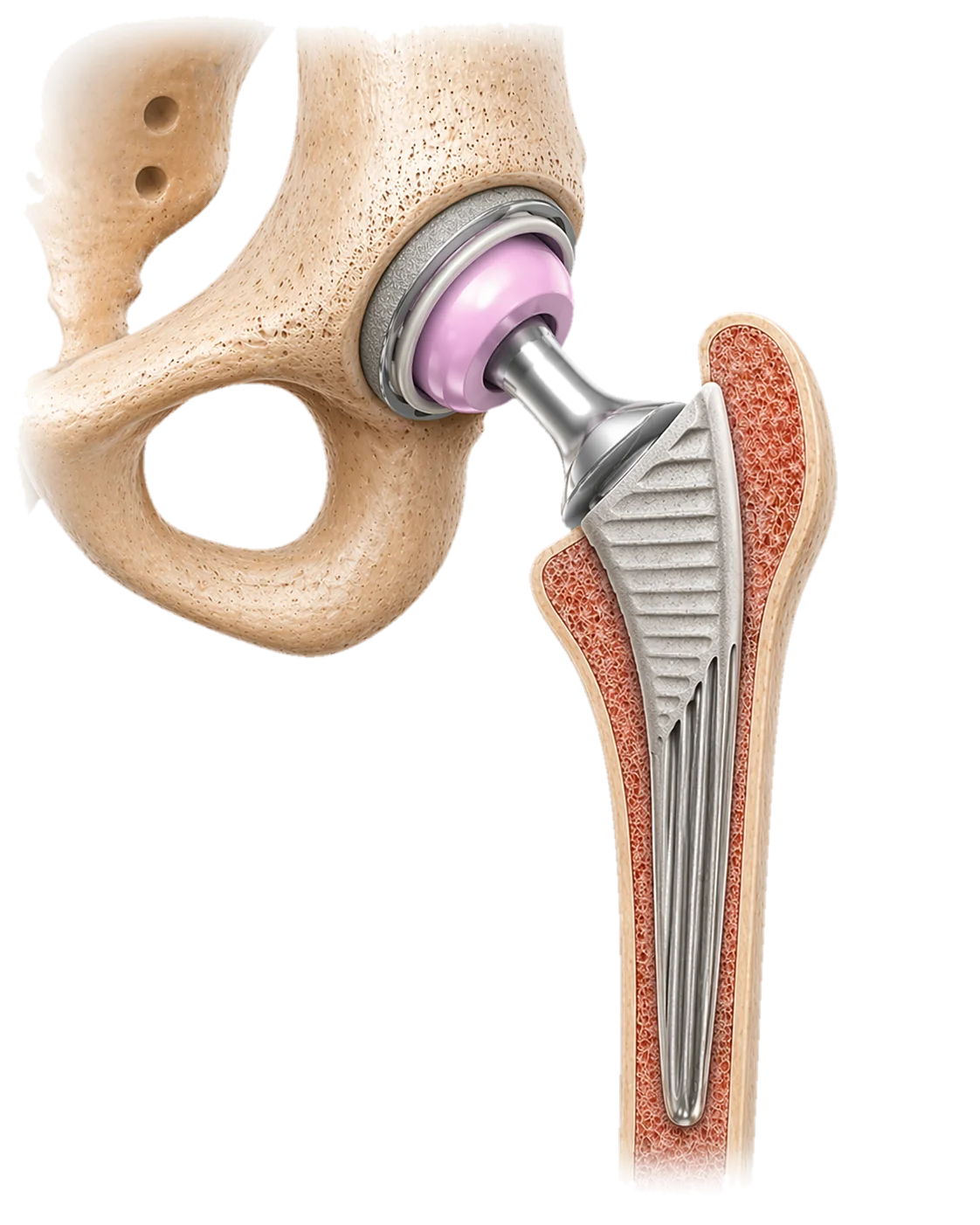
The worn femoral head is removed and replaced with a ceramic or metal ball on a titanium stem. The acetabular socket is resurfaced with a precisely-oriented cup and bearing liner.
A fluoroscopic image confirms implant position, leg length, and offset before closure, one of the key advantages of the anterior approach.
For patients who want the cosmetic result to match the clinical one, Dr. Debbi also offers the bikini variation of this same anterior approach. The operation underneath is identical, but the incision is placed obliquely, low in the natural crease of the groin, rather than running vertically down the front of the thigh.
Because it follows the natural grain of the skin, it tends to heal as a finer, flatter scar, and it sits low enough that ordinary underwear or a swimsuit covers it completely.
Learn more about the bikini incisionTimelines are typical, individual recovery varies based on age, health status, pre-operative condition, and adherence to physical therapy. Dr. Debbi will give you a personalized recovery plan.
Walked out of the hospital the same afternoon. Six days later I was off all pain meds and walking around Central Park. I had put this surgery off for two years, I wish I'd done it sooner.
Dr. Debbi explained every option, showed me my own CT scan, and told me honestly when I was and wasn't a candidate for certain approaches. The anterior hip was right for me. I was back on the tennis court at eight weeks.